"When many cures are offered for a disease, it means the disease is not curable" -Anton Chekhov
''Once you tell people there's a cure for something, the more likely they are to pressure doctors to prescribe it.'' -Robert Ehrlich, drug advertising executive.
"Opinions are like sphincters, everyone has one." - Chris Rangel
Hope Springs Eternal: Michael Fumento emails to say that the estimates for development of a SARS vaccine we see bandied about are wildly optimistic. For example:
A reliable test and possibly even a vaccine for the deadly SevereAcute Respiratory Syndrome (SARS) may be available within the next three to four years, predicts Anthony S. Fauci, the director of the National Institute of Allergy and Infectious Diseases (NIAID) at the National Institutes of Health, U.S. Department of Health and Human Service.
Replies Fumento:
By the time you've gone from discovery to rodents, then through all three phases, then await FDA approval you're talking five to seven years -- not three. Does Fauci not know this?
Has there ever been a disease for which a vaccine was developed in a few years? When you consider that the SARS virus is the same sort of virus that causes colds and that we don't have a vaccine or a treatment against colds, it pretty much dampens all enthusiasm for a drug treatment or a vaccine, at least in the near future. As this Wall Stree Journalarticle points out (subscription required):
Mutability is a family trait among RNA viruses such as the coronavirus that scientists have pinpointed as the cause of SARS. Unlike viruses whose genes are made of DNA, such as the hepatitis B virus, coronaviruses are chemically less stable and therefore more prone to make errors as they replicate, causing mutations.
That could have a big impact on world-wide efforts to keep the disease under control. For one, an effective SARS vaccine could prove much harder to produce. HIV is an RNA virus, and its constant mutation is one of the key reasons an AIDS vaccine has remained elusive. Another concern is that the disease may become more virulent as it changes. SARS has already killed about one in five people hospitalized with the disease in Hong Kong, according to a study released this week. posted by Sydney on
5/10/2003 09:09:00 AM
0 comments
Curtailing Costs:Work in Progress (scroll down a couple of posts) says that “cost cutting” in healthcare is actually care cutting:
The real problem is that what people calling for this want is to increase health care without increasing its costs. They want something for nothing. They keep hoping that someone will turn up with a magic pie that gets bigger every time you take a slice out of it.
There’s a lot to that. One of the reasons our healthcare costs are increasing is that the baby boomers have entered the age span when they need things like blood pressure medicine, cholesterol medicine, arthritis medicine, cardiac catheterizations, and colonoscopies. To be sure, there are some areas where costs can be cut - such as in the choice of drugs we use - but those cost savings aren’t going to occur as long as someone else is paying for them. posted by Sydney on
5/10/2003 08:31:00 AM
0 comments
Advance Apologies: For the next two to three months, posting will be much lighter than normal. My practice is undergoing a bit of sea change and it’s going to require more of my attention than it ever has before. So, if my posts are few, or if I’m slow to answer email or continue a debate, it’s not that I’m losing interest, just that there are other, more pressing (and more necessary) tasks to take care of first. posted by Sydney on
5/09/2003 08:38:00 AM
0 comments
Baghdad, Iraq, May 7 - Hundreds of Iraqi doctors, nurses and health workers demonstrated today against a decision by the American authorities here to appoint Ali al-Janabi, a senior Baath Party member, to be minister of health.
The demonstration by doctors in starched white coats was the latest indication of rising concern over the enduring influence of some members of the party that was long the vehicle for Saddam Hussein to impose his terror on Iraq.
The medical staff piled onto the bus that the American Third Infantry Division had provided to get them to their hospital jobs and told the driver to take them to the Baghdad hotel housing most foreign journalists. Unfurling neatly printed white banners, they marched silently, and a bit self-consciously, for the cameras.
"With this change in the country, we have the chance to give our ideas in a new democratic way," said Dr. Adel Eswet, a cardiac surgeon who helped organize the demonstration against the selection of Mr. Janabi, a senior official in Mr. Hussein's government. "So we're starting in a nice quiet democratic way."
Most of the health workers have not been paid in two months; many live without electricity and work in deplorable conditions. But that was not the reason for their anger. They came out in in a phalanx that was so neat and tidy that it looked more like a class photo than a protest. Indignation against the return of Baath Party officials powered their march.
Cells and Drugs: Go check out Derek Lowe. He's got a lot of great posts, from the development of cellular nanotechnology to recent progress in the treatment of amyloid diseases. posted by Sydney on
5/09/2003 08:36:00 AM
0 comments
True Grit: Been wondering how that Colorado hiker could amputate his arm with a pen knife? It wasn't easy. He says it was a cheap pocket-knife, and on his first try, it wouldn't even cut his skin, let alone his bones. So, here's what he did:
A day after his first attempt to cut his arm, Ralston went through the motions of applying a tourniquet, laying out bike shorts to use for padding. He worked out how to get through the bone with the "multi-tool"-type knife he carried.
"Basically, I got my surgical table ready," the 27-year-old said.
On the fifth day, he summoned up all his technique and nerve.
"I was able to first snap the radius and then within another few minutes snap the ulna at the wrist and from there, I had the knife out and applied the tourniquet and went to task. It was a process that took about an hour," he said.
I've read descriptions by soldiers and sailors of having their limbs amputated before anesthesia. They all say they passed out from the pain and couldn't remember anything about it. That guy must have had some will to live.
posted by Sydney on
5/09/2003 08:35:00 AM
0 comments
The results of the first clinical trial of an artificial retina implanted into the eye showed that it worked well enough to allow the blind to distinguish light from dark and even to see simple objects.
Each patient had an operation to have the implant fitted over their own damaged retinas. They wore spectacles fitted with miniature video cameras, which transmitted signals to the implanted device.
All the patients could see far better with the device switched on and one of them could even tell the difference between everyday objects.
State of Preparedness: The General Accounting office says that American hospitals would be unable to handle a SARS epidemic, or any epidemic, for that matter:
America's public health system — especially its front-line emergency rooms — is not ready for an outbreak of SARS or a similar infectious disease, according to a new government report and top trauma doctors.
"Most hospitals lack adequate equipment, isolation facilities, and staff to treat a large increase in the number of patients for infectious diseases such as SARS," the U.S. General Accounting Office reported Wednesday in testimony to the House Energy and Commerce Committee.
"We're way behind," GAO health care director Janet Heinrich said in an interview the same day.
And emergency room doctors, meeting in Washington said such an outbreak could collapse an already fragile American emergency room network.
"I liken the SARS problem right now to a two-acre fire in a tinder-dry forest," said Dr. Arthur Kellerman, an Emory University School of Medicine professor and Atlanta emergency room doctor. "We don't have the capacity in any city in my mind to handle a real outbreak of the disease."
The CDC counters that other places, like armories and hotels, could be used to house patients if need be, but the GAO still has its reservations:
But Heinrich said staff and equipment shortages at hospitals were so bad at seven cities visited by the GAO, Congress' investigative arm, that hospital officials said they would have trouble finding enough doctors and nurses to deal with an infectious-disease emergency. One state reported that only 11 per cent of its hospitals could expand enough to house and treat patients in such an epidemic.
I'd say that's about right. Every winter, we can count on a flux of hospitalized patients from the effects of influenza, yet every winter I often have trouble finding a hospital bed for my patients when they need to be admitted. And every winter, nearly every day, there's a sign posted on the door of the doctor's lounge at my hospital begging us to discharge patients as early as possible to help relieve the bed shortage. And that's when the surge is predictable. Hospitals just don't have a lot of unused beds lying around waiting for occupants. If they did, they'd go bankrupt in today's healthcare market. A real epidemic would break the system. posted by Sydney on
5/09/2003 08:12:00 AM
0 comments
Hah: How do you control healthcare costs? Ask the experts:
Medpundit Art History: There’s something hopelessly romantic about the mother-child relaltionship. No matter how ugly the reality of it can sometimes be, few of us can completely escape the temptation to idealize the love of a mother for her child.
And who better to idealize the ordinary than the Dutch masters? While previous generations of European artists specialized in translating the extraordinary tales of myth and religion into the ordinary, the Dutch genre painters of the 17th century specialized in translating the ordinary into the extraordinary.
Citizens of a newly formed Protestant nation that gloried in its hard won independence from Catholic Europe, they painted not for rich nobles, but for the common man. Their patrons were their fellow citizens, the bankers, farmers, and merchants, were willing to pay fair market value for their work. Not surprisingly, those same citizens, and their possessions, were the most popular subjects.
Painted around 1660 by Gabriel Metsu (1629-1667), Mother with Sick Child portrays in intimate detail a moment in the life of an ordinary mother and child. Once past infancy, children rarely sit still long enough to be held so totally in their mothers’ arms, unless they’re tired. Or sick. And it’s those moments that hark back to the days of infancy, when no personality conflicts or power struggles have yet to rear their heads. When both mother and child are starting with a blank slate. And when most mothers are willing to subsume all other concerns to the needs of their child. It is at such moments that the love of a mother for her child comes closest to the ideal.
Here, the mother holds her child in a pose that would have been quite familiar to his audience. We can’t see her face since she's completely absorbed in her child, but her demeanor seems one more consistent with calm scrutiny rather than alarm or anxiety, as if she’s objectively evaluating the severity of her child’s illness. Or perhaps she's trying to decide how best to get the medicine (or soup) in the bowl at the lower left corner into her offspring. The child, her sickness not severe enough to kill her curiousity looks straight at the viewer. Her languid attitude suggests that perhaps she just has a slight fever and her mother has undressed her in an attempt to cool her down.
Yet, in those days of smallpox, plague, and untreatable bacterial infections, every fever was a potential harbringer of death. Only time would tell what would prove to be a minor illness and what would be fatal. And this specter of death hovers in the picture, too. The mother's blood red skirt flows out from the child's side as if from a wound. The child's petticoat drapes across her lap like a shroud. On the wall behind the pair, to the right, hangs a dark painting of the crucifixion. Just barely discernable in its shadows is the figure of a woman in sorrow kneeling at the feet of her dying son. Which, in turn, brings to mind yet another familiar image of a mother and her suffering child echoed in the painting, reminding us that it's in ordinary moments like this that we come closest to perfect love.
Preparedness: What the US is doing to prepare against SARS:
The Centers for Disease Control and Prevention in Atlanta is purchasing 3,000 ventilators used for isolating SARS patients. They will be added to the nation's emergency stockpile of medical supplies set up to respond to a terrorist attack or other major event involving mass numbers of victims, said Dr. Julie Gerberding, CDC's director.
The new ventilators will be used to supplement the 100,000 ventilators already in the stockpile, Gerberding said.
If the number of U.S. SARS cases increases rapidly, the CDC's first response would be to "act fast," implement quarantines and shut down affected hospitals, she said. The saving grace would be that SARS is "not nearly as infectious as influenza" so it would not spread as rapidly, she added.
....The Food and Drug Administration also has "taken a number of steps to address a possible escalation of SARS cases in the United States," said Dr. Murray Lumpkin, the FDA's principal associate commissioner.
These include putting the necessary regulations in place so experimental medications could be used in an emergency even if the therapies do not yet have full FDA approval, Lumpkin said.
The FDA also is trying to expedite the development of a diagnostic test that can detect whether people are infected with the SARS virus and working with the public and private sector to develop a vaccine and identify potential medications that block the virus.
The agency also has provided an exemption to the approval requirements for CDC so it can get its diagnostic test out more rapidly to labs around the country to help with diagnosing potential SARS patients, Lumpkin said.
The National Institutes of Health in Bethesda, Md., are working to develop a vaccine against SARS, but it probably will take "a couple of years at least," said Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, a component of the NIH.
Interesting, that bit about shutting down hospitals. A lot of hospitals are running on pretty thin margins. That could bankrupt them, since unlike Canadian, Chinese, and Hong Kong hospitals, American hospitals, with very few exceptions, aren't financed by the government.
More SARS: And on the mortality rate debate, Michael Fumento sent along this article about yesterday's SARS death rate news, noting that the study probably suffers from selection bias:
The first major study of SARS trends estimates that about 20 percent of the people hospitalized with the disease in Hong Kong are dying from it, but some experts believe the number is skewed because of the patients' ages.
The average age of the Hong Kong patients is 50, and disease experts generally agree that the virus is much more deadly in people over 60. In fact, the new study puts the death rate for those over age 60 at 55 percent.
The findings of the study, published yesterday on the Website of The Lancet medical journal, are similar to earlier, cruder estimates for Hong Kong, one of the areas hardest-hit by SARS.
However, experts warn that the figures do not reflect the chances of the average person anywhere dying from a bout of SARS once they have contracted it.
It also appears to be quite a bit lower in countries where the epidemic has played itself out:
But WHO officials noted that the death rate is lower in places where the outbreak has ended or is nearing an end. "We know that in a real situation where the outbreak has completed itself from beginning to end - in Hanoi, Vietnam - they had an 8 percent case fatality rate," said WHO spokesman Dick Thompson.
That would agree with the New England Journal of Medicine'sfigures. (scroll down past the article links)
Fumento also noted that the author of Lancet article (see yesterday’s post) has a reputation for scary epidemiology, especially when it comes to things like heterosexual AIDS transmission. And, Fumento has more on SARS scare statistics at NRO. posted by Sydney on
5/08/2003 07:54:00 AM
0 comments
Two hospitals in have reported 17 confirmed cases of cholera in the Iraqi city of Basra, and the World Health Organization said Wednesday it fears far more have gone unreported.
A WHO team dispatched to the southern city this week said the number of confirmed cases of cholera does not reflect the extent of the disease.
"An outbreak of cholera, affecting probably several hundreds of people, is occurring," said WHO spokeswoman Fadela Chaib.
The first confirmed cases in Basra turned up in children age 4 and under. Tests were done by the Al-Tahir Teaching Hospital and Basra Maternal and Child Hospital.
Additional samples have been sent to a laboratory in Kuwait for confirmation, and results are expected by Thursday.
Seventeen cases does not an epidemic make, although poor sanitation and unclean water do make the situation ripe for it. However, it's not clear that things are as bad as the article makes it sound:
British forces and aid agencies have sent water tankers through the city and surrounding towns, and British engineers have restored about 80 percent of the water system.
Not only that, it turns out that cholera is common in Iraq:
Local doctors say cholera outbreaks occur each year in southern Iraq but with the medical system under a huge strain treating war injuries, they fear this one may be worse.
And apparently Uganda wishes it only had seventeen cases of cholera:
"We have recorded 601 cases of cholera, with 44 deaths, in the district between January 5 and April 20," Bundibugyo Resident District Commissioner Erasto Gubaare told AFP news agency.
Multiply that by the WHO official's factor of ten and that is, indeed, an epidemic. But evidently, no one's paying any attention:
"International agencies should come to the rescue of these people," the health official added.
Are there any international agencies not preoccupied with exaggerating the plight of post-war Iraq WHO could help these people? posted by Sydney on
5/08/2003 07:10:00 AM
0 comments
Trust Me, I'm a Doctor: Writing on NRO, James Lacy says that there's little evidence of civilian casualties in Iraqi hospitals, despite what doctors tell reporters:
I asked the only female doctor present how many patients they had treated who had been injured in the fighting, and how many of them were men. She replied that they had treated about 600 patients and that they were mostly men. Dr. Ali quickly corrected her and they began to argue in Arabic. He then announced that it had been about half men and half women.
Dr. Ali insisted on being my escort for the remainder of the visit. He explained that the hospital's fifth and sixth floors were reserved for civilians who had been injured in the war. Men were on the sixth floor, women and children on the floor below.
The first room off the elevator was filled with the men who had suffered the worst injuries. None of them spoke as the doctor showed me each of their many wounds.
I went from room to room without saying a word. It was hard to look at the broken bodies lying in such unsanitary conditions, but I also noticed something else. There was only one man who seemed to be over age 40 on the entire floor. Of the 46 patients I counted, 45 appeared to be in their early twenties.
When I visited the women's and children's floor, most of the rooms were empty. Besides Esraa and Nor, there was only one middle-aged woman, who had been wounded in the side by shrapnel. She also was expected to make a full recovery.
I asked Dr. Ali why, if these were all civilian casualties, there was not an even distribution of males and females and among age groups. Why did the overwhelming number of them appear to be men of military age? He offered no explanation, but continued to insist that the men were all civilians. He then added that many civilians had been killed, too, and I should check the morgue and see.
When I did try to check the morgue, they would not allow me to see any of the wrapped bodies, but did let me go through the paperwork. At my request, a clerk pointed out where the name was supposed to be on each form. Most of the name blocks were blank. Pressed for an explanation he said, "They are not known here." It was only then that it struck me that most of the men lying in the hospital had no family around them — unlike Esraa and Nor, who were surrounded by family members. The clerk's statement probably meant that these men were fighters from Baghdad, who had no relatives in Najaf.
It should come as no surprise that Iraqi doctors are prone to exaggerating the extent of American-caused casualties. In a totalitarian regime, those people who embrace the party-line are the ones who get ahead. This is true in all walks of life, not just politics. And it's especially true in fields that require an education in state schools. This happened in Nazi Germany, too. So why aren't reporters more skeptical of Iraqis in positions of authority? Especially after they've witnessed scenes like this?
Turns out things aren’t so bad in Baghdad, either :
There are more hospital beds available in Baghdad than there are patients to fill them, the U.S. officials said late last week.
The International Committee of the Red Cross provided some independent backing for that claim, reporting that the 250-bed Al Na'uman hospital had 90 patients.
"The staff are generally less busy now, and carry out five to six surgical interventions a day," the report said.
...Doctors at two Baghdad hospitals — one state-run and the other private — said in interviews that their main business was attending to people with gunshot wounds or burns caused by antilooter and antitheft vigilante activities, score-settling, handling of unexploded ordnance and general lawlessness.
..."The unfortunate part, the problem we have, is we continue to get these offers and donations that really overwhelm the system," she said.
"Drugs and medications get outdated. The amount is just too much," she added. "We have enough crutches and bandages to last us 10 years."
...The most important medical need in Iraq now, officials said, is to vaccinate children younger than 5. One in three Iraqi children of that age has not been immunized, whereas almost all children of the same age in neighboring states have had the vaccinations
If they have the time and energy to turn their attention to preventive medicine, then things can't be all that bad. And notice that those children haven't been immunized in the past five years. Just what were they doing before the fall of Baghdad? It suggests that the state of medicine may actually be improving in Iraq since the liberation, rather than declining.
posted by Sydney on
5/07/2003 08:00:00 AM
0 comments
Medicine in the Anglosphere: A recent survey within the Anglosphere shows that a quarter of patients have experienced medical errors:
The Harvard survey of sick adults was conducted in the United States, Canada, the United Kingdom, Australia and New Zealand. At least 750 persons were surveyed in each country.
The United States had the highest portion reporting errors -- 28 percent -- and the United Kingdom the fewest, 18 percent. But in all five countries, those who went to more than two doctors complained of errors almost twice as much as those who went to just one or two physicians.
...''This is only 10 percent of patients,'' he said, ``but they're an expensive 10 percent.''
The survey showed that more than one in four -- 28 percent -- of those who see more than two doctors in the United States and Canada said they were given duplicate tests by different doctors. And roughly a quarter in all five countries said they received conflicting information from different doctors.
One of the experts interviewed in the article suggests that paying for “case managers” to coordinate care would help prevent these sort of errors. You know, there are people out there who do this now. They’re called primary care physicians.
But Florida has come up with unique plan to reduce medical errors:
Last week, the Florida Legislature, attempting to cut down on medical errors, passed a bill ordering doctors to improve their handwriting, so that pharmacists and nurses could do a better job of reading prescriptions.
Payouts: The crux of the malpractice insurance crisis:
The bulk of the dollars the insurers pay out in malpractice cases is in the form of settlements, not verdicts. In 2002, the year insurance carriers in New Jersey lost only 54 cases, they settled 732. Jury awards, Leone explains, put floors under the amounts for which suits can be settled. If juries have tended to award plaintiffs $1 million for a certain injury, the insurer knows it can't expect to settle a similar case for much less.
And the direction of verdicts and settlements, Leone claims, is up. In 1998, he says, Princeton's average payment to plaintiffs in malpractice cases against doctors was $235,000; in 2002 it was $343,000. The company's total payout to physician malpractice plaintiffs rose from $88 million in 1998 to $115 million in 2002.
Not to mention the money they spend reaching those settlements.
Speaking of Settlements: A while ago, when I posted a rant about lawyers seeking out injured clients, I got a barrage of email from lawyers who said this was not a common practice and that any lawyer who solicited clients would be disbarment material. Well, take a look at this story about people who make their living chasing down accident victims for lawyers:
Big business. Ask attorney David Shurtz. Each year, he pays out at least $100,000 to runners for referrals.
"Most of these people do not have anything beyond a high school diploma, and I know at least one of my investigators made $30,000 in a month," says Shurtz. (That's 50 cases at $600 apiece -- an extraordinary hustle.) Some of the runners are former clients. One was Shurtz's receptionist, who wised up, he says, when she realized she could make better money in fewer hours.
"I'm not ashamed of it," Shurtz says. "It's ethical. And if my greatest sin is giving $100,000 back to guys with high school diplomas who are out there working hard bringing in cases, send me to the gallows."
.....Personal injury cases can be sold to a lawyer for $300 to $600, sometimes more if the victim broke some bones or died. Not bad money. (They deal mostly in soft-tissue injury cases, which often get settled out of court, with the client netting a few thousand dollars.) Some runners say they can make $50,000-plus a year. Johnson estimates a runner can make up to $100,000.
...Some runners also offer money to potential clients to get cases.
"If I can get all of you signed up today, I'm offering all of you $150 apiece, that's cash money in your pocket," says one of the Fuddruckers lunchers while making phone calls in her car. She's just come out of the 5th District station with a notebook of names and numbers, including this bonanza: a vehicle that had three people in it when it was hit. That's enough business to justify $450 from her pocket.
"Solicit" must have a different meaning in legalese than it does in English.
SARS Epidemiology: The Lancet publishes the first study of SARS epidemiology today (online). The mortality rate appears to be quite a bit higher than the 4 to 8% we've been hearing:
The mean incubation period of the disease is estimated to be 6.4 days (95% CI 5.2-7.7). The mean time from onset of clinical symptoms to admission to hospital varied between 3 and 5 days, with longer times earlier in the epidemic. The estimated case fatality rate was 13.2% (9.8-16.8) for patients younger than 60 years and 43.3% (35.2-52.4) for patients aged 60 years or older assuming a parametric g distribution. A non-parametric method yielded estimates of 6.8% (4.0-9.6) and 55.0% (45.3-64.7), respectively.
Yet, no one in the United States has died from the disease, and worldwide the mortality is much lower. (See the New England Journal of Medicine'sgraph.) I suspect that the key to survival is to get early treatment. Even though there's no known drug treatment, early supportive care, such as ventilators and oxygen, probably make the difference. posted by Sydney on
5/07/2003 07:20:00 AM
0 comments
Tuesday, May 06, 2003
Alt Med Update: The wonderful world of herbal supplements has taken a hit in Australia. One company has had to recall hundreds of its products over safety and quality concerns:
More than 200 products were recalled in Australia this week when an audit revealed the company's breach of safety standards.
The problem widened last night when Australia's drugs watchdog added a further 449 products to the recall list.
That makes 668 products with possible health risks - and the Therapeutic Goods Administration indicated the list could reach 1000.
Pan is accused of substituting ingredients, manipulating test results and having substandard manufacturing processes.
Proving once again that herbal supplements are just as risky as any other drug, here's a description of one of the adverse reactions from taking the company's travel-sickness supplement:
The decision to withdraw all the company's products was made after 19 people were hospitalised after taking the travel medication Travacalm and dozens of others reported adverse reactions, including hallucinations that led to users attempting to jump out of the planes they were in. posted by Sydney on
5/06/2003 08:32:00 AM
0 comments
Friendship Means Sharing: Had to chuckle at the footnote to this SARS story:
A 60-year-old Gainesville woman, whom authorities declined to name, returned to Gainesville in late March after a visit to Beijing. She had a cough, but did not seek medical treatment until after she had coughed near a co-worker, a 47-year-old woman, whom she infected.
Both women were hospitalized in early April but have since fully recovered, according to Thomas Belcuore, health director for Alachua County. Neither showed signs of pneumonia and both are therefore still classified as suspect, rather than probable, SARS cases. They remain friends, Belcuore said.
Lessons: Ontario is taking the lessons learned by SARS to heart:
Ontario will launch a major overhaul of its hospital operations in the wake of the SARS outbreak, forcing changes in everything from basic infection control to the use of casual nursing help, Tony Clement, the Health Minister, said.
"We want to make sure that as a result of what I call the 'new normal,' our hospital system continues to be of the highest quality," Mr. Clement said in an interview. "Some aspects of hospital operations have changed forever."
The changes include less use of part-time nurses who work in several hospitals at a time, less transfer of patients between hospitals, and the recognition that hospitals need a "surge capacity" to handle unexpected epidemics. That's something hospitals here in the U.S. would do well to recognize, too.
And, as familiarity with SARS grows, so does our understanding of its natural history. Looks like it’s one of those viruses that can survive outside the body:
New laboratory findings support the theory that the SARS virus can survive up to four days on contaminated household surfaces like toilets but that disinfectants like bleach are effective weapons to kill it, the World Health Organization said yesterday.
The findings are important because doctors have determined that people infected with the virus can excrete it in large amounts in their stool and urine, raising the distinct possibility that less than vigorous hygiene - particularly a lack of hand-washing - can lead to its spread on surfaces in the home and elsewhere.
Health officials had assumed that this must be the case because of the pattern of spread in an apartment complex and hotel in Hong Kong. The new findings strengthen the theory, said Dr. Klaus Stohr, a German virologist and epidemiologist who is the scientific director of the W.H.O.'s SARS investigation.
Researchers at The University of Hong Kong found that disinfectants like bleach, ethanol, phenol, formaldehyde and paraformaldehyde can kill the virus, the W.H.O. said.
The findings should give further confidence that such measures, particularly in hospitals and homes where people who had contact with SARS patients are quarantined, will work, Dr. Stohr said in an interview.
The rest of the article has all the details on the viruses survival at various temperatures as well as its survival in various qualities of stool. (I don't envy the people doing those studies.)
But, the LA Times points out that it’s still unclear how all of this translates into communicability:
Stohr cautioned that the full meaning of the findings will not become clear until researchers learn how much virus is necessary to trigger an infection. That the virus can persist for hours on, say, handrails in a bus station may not be important if there is not enough of the virus present to produce disease....
.....Scientists remain convinced that the main way the disease is spread is through the coughs of patients. The greatest danger is thus to people in their immediate vicinity.
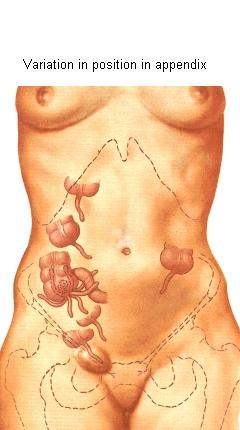
Not so Obvious: A reader recently emailed wondering about appendicitis, and how hard it is to diagnose. A couple of his friends had recently suffered the consequences of a delay in diagnosis - commonly referred to as a “ruptured appendix.” (It doesn’t really burst like a balloon. It’s just that the infection spreads beyond the appendix to the surrounding organs and abdominal cavity, a much more severe condition known as peritonitis.)
As it turns out, appendicitis isn’t always as straight forward as it would seem. A textbook case begins as pain around the belly button and progresses to a more localized pain in the right lower abdomen, accompanied by a lack of appetite. Often, there’s also vomiting, constipation, and fever. However, our bodies don’t read the textbooks.
The appendix, a worm-like appendage of dubious usefulness, usually hangs straight down from the first portion of the large intestine, the cecum. However, like so many other things biological, the position of the appendix, and of the cecum within the abdominal cavity can vary widely. When an appendix sitting in a “normal” position gets infected and inflamed, it causes the classic textbook symptoms of right lower abdominal pain and tenderness. This, however, only happens about fifty percent of the time. An appendix sitting behind the obturator muscle causes a pain sensation in the pelvis, sometimes only detected with a rectal exam. An appendix behind the psoas muscle causes side pain. Sometimes, it hides behind the cecum, causing only mild pain in response to the doctor’s probing hands on the abdomen. In pregnant women, it gets even harder since the appendix can be displaced just about anywhere and shielded from examination by the enlarged uterus.
And, to complicate matters, most abdominal pain does not turn out to be appendicitis. Ovarian cysts, urinary tract infections, gastrointestinal viruses, and kidney stones, to name just a few, can present in a similar manner. And, since surgery is a risky business, doctors only like to operate if the likelihood of appendicitis is fairly high.
So, we're constantly searching for something that will increase our diagnostic certainty. Looking for higher numbers of white blood cells in the blood than usual is helpful, but not a certain indicator of appendicitis. Ultrasound can sometimes help to identify an enlarged and inflamed appendix, but it can miss cases, too. The state of the art at the moment is to use helical CT scans when in doubt. They give a high-resolution picture of the appendix that can pick up inflammation in surrounding tissue even at early stages. And, most importantly, they can identify a normal appendix.
If diagnosed within the first twenty-four to thirty-six hours, the surgical cure is relatively straightforward and simple. These days, it can be done laparoscopically, which means fewer surgical complications and a faster recovery time. Usually, patients go home the day after surgery if all goes well, leaving their appendices behind them.
Great Names: A physician in Britain named Marcus Aurelius recently passed away. Marcus Aurelius was the Roman emperor who financed Galen, the father of modern medicine. posted by Sydney on
5/05/2003 08:32:00 AM
0 comments
SARS Update: This week’s Lancet (free registration required) is full of SARS news. Turns out the disease is less severe in young children for some reason.
It also turns out that respiratory droplet precautions (masks, gloves, handwashing) are essential in preventing the spread of the disease:
All participants were surveyed about use of mask, gloves, gowns, and hand-washing, as recommended under droplets and contact precautions when caring for index patients with SARS. 69 staff who reported use of all four measures were not infected, whereas all infected staff had omitted at least one measure.
Maybe Chuck Simmins is right, after all. Sloppy precautions on the part of hospital staff members may have played a critical role in the disease’s spread. posted by Sydney on
5/05/2003 08:24:00 AM
0 comments
What's in a Name? William Safire has dug up the origin of SARS:
Here is how SARS the acronym came about. Three worried officials of the World Health Organization in Geneva, Switzerland, needed a name for a virus causing sudden deaths in China. The three were Denis Aitken, deputy director general; David Heymann, director of the Communicable Diseases Section; and Richard Thompson, its communications officer. (Presumably, he answers the phone with ''Communicable communications here.'')
''We wanted a name that would not stigmatize a location,'' Thompson says, ''such as 'the Hanoi Disease.' We first thought of A.P.W.D., or Atypical Pneumonia Without Diagnosis, and I'm glad we dropped that. Then we simply described the disease in another way, and it was in front of us -- Severe Acute Respiratory Syndrome, SARS.''
But what did they see as the difference between severe and acute?
''I asked this question, too, when we came up with the name. In medicine, severe is 'grave' and acute means 'suddenly.' This respiratory syndrome caused great harm (severe) and had a rapid onset (acute). Later, when we had conclusive evidence that a new coronavirus is the cause of the disease, we named it the SARS virus.'' posted by Sydney on
5/05/2003 08:15:00 AM
0 comments
Office Manners: I missed the essay in the Cleveland Plain Dealer that led to these letters to the editor, but evidently it was about encounters with doctors of the brief kind. This one struck a chord:
For a couple of years, I have noticed a new rival during office visits: The computer.
About 90 percent of my visit time is spent watching the doctor type into a desktop computer. The doctor sits facing the terminal, not looking at the patient, and type-type-types, with a few seconds of time-out every once in a while to ask me a question. Before I finish answering, the doctor has turned back to the terminal and types some more.
It's like having another person in the room who is getting all the attention, and I hate it! I feel like saying, "Excuse me, are you here today?"
If only that were unique to computers. I sometimes find myself doing the same thing with pen and paper. Unlesss it’s a straightforward encounter, I have to write down what the patient is telling me, or I’ll forget. Sometimes there’s just too much information coming at once to trust my brain; sometimes it’s things that are out of the ordinary. It’s so easy to get side-tracked, you wouldn’t believe. And memory is such a tricky thing - for patients and doctors. It’s much better sometimes to sacrifice politeness for accuracy. posted by Sydney on
5/05/2003 08:12:00 AM
0 comments
Public Health Militancy: Last week the New York Times ran an interesting graphic on its editorial page that showed the relative incidence of deaths from various diseases around the world. SARS occupied a tiny portion when compared to diseases like tuberculosis. (Unfortunately they didn’t make it available on the internet. Probably took up too much bandwith.) It illicited this response from one reader:
Howard Markel and Stephen Doyle present the real problem. The diseases enumerated demonstrate that our focus should be on public health, saving countless more lives than all the regime changes in the world.
Ah, but here’s the rub. Those diseases, like tuberculosis and HIV, are killing people in large numbers in nations with chaotic governments. Nations where the leaders live well and the people live miserably. (see the post below re: life expectancy) Nations where leaders starve their people for political reasons. You can hardly expect those governments to embrace public health measures to cut infectious disease. Which means that if those diseases are to really be eliminated, it would take a regime change. posted by Sydney on
5/05/2003 08:00:00 AM
0 comments
Apologies: No blogging today. The day was too beautiful to spend at the computer. Blogging resumes tomorrow. posted by Sydney on
5/04/2003 10:26:00 PM
0 comments





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}