"When many cures are offered for a disease, it means the disease is not curable" -Anton Chekhov
''Once you tell people there's a cure for something, the more likely they are to pressure doctors to prescribe it.'' -Robert Ehrlich, drug advertising executive.
"Opinions are like sphincters, everyone has one." - Chris Rangel
Bad reporters find experts by calling up university press relations officials or brokerage research departments and saying, in effect, "Gimme an expert"; some academic publicity machines send out rosters, complete with phone numbers, e-mail addresses and areas of expertise, so that the lazy journalist doesn't even have to make that first call. Really bad reporters, paradoxically, work a little harder: knowing the conclusions they want to arrive at, they seek out experts who just happen to agree with them. Give me a position, and I'll find you an expert to support it - and not just an expert but one with an institutional affiliation sounding so dignified it could make a nobleman genuflect. Give me a Center for the Study of ..., an Institute for the Advancement of ..., or an American Council on ..., and often as not I'll give you an organization whose special interests are as sharply defined as its name is not.
He's talking about experts that get quoted in the news, but the same applies to those "expert witnesses" in our court system. posted by Sydney on
10/30/2004 09:32:00 PM
1 comments
UPDATE: Slate's Fred Kaplan says the Lancet paper's numbers are a dart board, not an estimate. Regarding the 100,000 "estimated" Iraqi civilian deaths since the war:
The report's authors derive this figure by estimating how many Iraqis died in a 14-month period before the U.S. invasion, conducting surveys on how many died in a similar period after the invasion began (more on those surveys later), and subtracting the difference. That difference—the number of "extra" deaths in the post-invasion period—signifies the war's toll. That number is 98,000. But read the passage that cites the calculation more fully:
We estimate there were 98,000 extra deaths (95% CI 8000-194 000) during the post-war period.
Readers who are accustomed to perusing statistical documents know what the set of numbers in the parentheses means. For the other 99.9 percent of you, I'll spell it out in plain English—which, disturbingly, the study never does. It means that the authors are 95 percent confident that the war-caused deaths totaled some number between 8,000 and 194,000. (The number cited in plain language—98,000—is roughly at the halfway point in this absurdly vast range.)
This isn't an estimate. It's a dart board.
Imagine reading a poll reporting that George W. Bush will win somewhere between 4 percent and 96 percent of the votes in this Tuesday's election. You would say that this is a useless poll and that something must have gone terribly wrong with the sampling. The same is true of the Lancet article: It's a useless study; something went terribly wrong with the sampling.
MORE: The blog Ragout, points out that the statistician mentioned in the Slate article is doubly credible. She's not only experienced in Iraqi civilian mortality rates, she was fired by the first Bush administration because they thought her numbers were too high after the first Gulf War. If she thinks the Lancet study is fishy, it's fishy. posted by Sydney on
10/30/2004 08:40:00 AM
0 comments
Friday, October 29, 2004
Call for Grand Rounds: Just a reminder that submissions for next week's Grand Rounds should be sent to medpundit-at-ameritech.net (or just click the email link in the left hand column) by Monday, Nov. 1, at 9PM. Any health or medical-related topic is welcome, as are non-medical bloggers. posted by Sydney on
10/29/2004 08:31:00 AM
0 comments
The researchers, from the University of Santiago de Compostela, compared the lifestyles of 132 patients with lung cancer to 187 patients without lung cancer who had minor surgery at the same hospital in Spain between 1999 and 2000. In both groups, nearly 90 percent of the subjects were men.
Both groups drank similar amounts of wine, about 3.5 glasses a day, the researchers found. (U.S. health experts caution that moderate drinking for optimal health is defined in general as one drink a day for women and two for men.).
The researchers found that each daily glass of red wine reduced the risk of lung cancer by 13 percent. Rose wine had no effect and white wine seemed to raise the risk, although the researchers said not many of the subjects drank white wine. Beer or spirits had no apparent effect on lung cancer development.
It isn't a very well-designed study. Comparing a group of lung cancer patients with a group of people without lung cancer and just comparing their lifestyles doesn't even begin to approach preciseness. There could be many uncontrolled variables that are effecting the results, other than wine drinking. I wouldn't count on the bottle to counteract an post-prandial cigarette. posted by Sydney on
10/29/2004 08:16:00 AM
0 comments
Pulse of the People: Only four more days until election day, and I'm beginning to detect a shift toward Bush among my patients. No one comes in wearing Bush/Cheney buttons, but no one comes in wearing Kerry/Edwards buttons anymore, either, unlike a couple of months ago when just about every union member wore one. In fact, the only guy wearing a campaign button recently was a union member wearing a "Veterans for Bush" button.
There are other signs that support is swinging toward Bush. One of my patients, as he was leaving, turned to me and said, sotto voce, "You know Kerry has never once voted for tort reform, don't you?" (Yes, I know.) Another patient tells me how anxious he's feeling after the first debate. He's worried about what a Bush defeat would mean. A woman asks me if Bush is responsible for the flu vaccine shortage, then cuts me off before I can answer because she'd vote for him anyway. "There are more important things than flu vaccines."
But yesterday's patient was the tipping point. Mr. B. is an elderly academic. You would know that just by looking at him. He carries an NPR tote bag, and reads Snail Magazine. He's a jazz afficionado, and travels to France every year to share that love with others. He speaks very carefully in a very p.c. manner. He happened to be in my office on September 11, 2001, and I very clearly remember him fretting about the effect of globalization and modernity on the world. A Kerry voter if ever there was one. Or, at least so I thought. But he has developed one of those diseases that forces a person to re-assess his life. Yesterday, he was explaining to me how his disease had made him re-examine his core beliefs, many of which he had suppressed for many years to succeed in academia. And in the midst of a discussion (or really a soliloquy, he's a professor, after all) about God and man and reason, he suddenly digressed to Vietnam, saying, in effect, it was foolish to think we could reason with the North Vietnamese. And he stopped suddenly, as if he had just shocked himself. Now, he didn't mention the election. He didn't mention Kerry's suppression of his own faith to his political ambitions, or Iraq, or the war on terror, but he gave me the impression that although he was talking about Vietnam, he was really thinking about the war on terrorism, and the war in Iraq. I bet when the curtain closes behind him on Tuesday, he punches the card for Bush. Maybe I'm wrong, but the fact that a man with his background is even rethinking these long-held beliefs is significant.
posted by Sydney on
10/29/2004 08:14:00 AM
0 comments
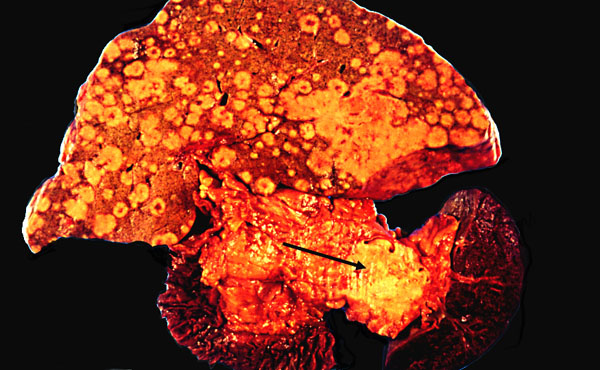
Palestinian Leader Yasser Arafat was scheduled to fly to Paris early Friday for emergency medical treatment after his health declined sharply in recent days and teams of international doctors were unable to diagnose his ailment, according to a senior Palestinian official.
"All his doctors agreed that he needs a hospital, some place where all kinds of tests can be made safely," said Palestinian Foreign Minister Nabil Shaath.... Shaath described Arafat as "very weak, frail and pale."
Arafat, 75, has been sick for about a week and has been examined and treated by doctors from Tunisia, Egypt and Jordan. Doctors and aides have described his illness variously as a severe flu, an intestinal infection and gallstones. Earlier this week, doctors said he underwent an endoscopy to examine his digestive tract.
Israeli intelligence officials have speculated that he has stomach or colon cancer, which Palestinian officials have denied.
....Arafat's spokesman, Nabil Abu Rudeineh, told reporters early in the day that the Palestinian leader was "in stable condition, but he is still in need of more rest and more medical care." He would not discuss the nature of Arafat's illness or provide any details, other than to say Arafat had not lost consciousness.
"The president is seriously sick," said Mustafa Barghouti, a Palestinian political analyst and reform advocate who was among the visitors to the compound. "He has had serious problems with his gastrointestinal system. He has not been able to eat, and he's been vomiting."
But Arafat aides said the Palestinian leader, who spends much time dozing, often suffers memory loss and cannot recognize the people around him, even his bodyguards.
And reports that his platelet count is low, when considered with this picture in which he looks jaundiced, his face emaciated, but his belly bulging - all suggest liver failure. He's 75. My money is on cancer with liver metastases. posted by Sydney on
10/28/2004 09:58:00 PM
0 comments
or the first time in its history, the Centers for Disease Control and Prevention has created a permanent panel of ethicists on vaccine distribution, to help navigate the life-and-death questions of who should get flu vaccines in the current crisis and how the agency should cope with any future epidemics.
"Ethicists have unique tools to help shape our decisions,'' Dr. Julie L. Gerberding, director of the C.D.C., said in an interview yesterday. "We want to make sure that whatever we decide is equitable.''
Translation: I don't want to take the heat for the decision.
Physician, Heal Thyself:The New Yorker looks at high drug prices and says the problem is volume:
The second misconception about prices has to do with their importance in driving up over-all drug costs. In one three-year period in the mid-nineteen-nineties, for example, the amount of money spent in the United States on asthma medication increased by almost a hundred per cent. But none of that was due to an increase in the price of asthma drugs. It was largely the result of an increase in the prevalence of usage—that is, in the number of people who were given a diagnosis of the disease and who then bought drugs to treat it. Part of that hundred-per-cent increase was also the result of a change in what’s known as the intensity of drug use: in the mid-nineties, doctors were becoming far more aggressive in their attempts to prevent asthma attacks, and in those three years people with asthma went from filling about nine prescriptions a year to filling fourteen prescriptions a year. Last year, asthma costs jumped again, by twenty-six per cent, and price inflation played a role. But, once again, the big factor was prevalence. And this time around there was also a change in what’s called the therapeutic mix; in an attempt to fight the disease more effectively, physicians are switching many of their patients to newer, better, and more expensive drugs, like Merck’s Singulair.
Asthma is not an isolated case. In 2003, the amount that Americans spent on cholesterol-lowering drugs rose 23.8 per cent, and similar increases are forecast for the next few years. Why the increase? Well, the baby boomers are aging, and so are at greater risk for heart attacks. The incidence of obesity is increasing. In 2002, the National Institutes of Health lowered the thresholds for when people with high cholesterol ought to start taking drugs like Lipitor and Mevacor. In combination, those factors are having an enormous impact on both the prevalence and the intensity of cholesterol treatment. All told, prescription-drug spending in the United States rose 9.1 per cent last year. Only three of those percentage points were due to price increases, however, which means that inflation was about the same in the drug sector as it was in the over-all economy. Angell’s book and almost every other account of the prescription-drug crisis take it for granted that cost increases are evidence of how we’ve been cheated by the industry. In fact, drug expenditures are rising rapidly in the United States not so much because we’re being charged more for prescription drugs but because more people are taking more medications in more expensive combinations. It’s not price that matters; it’s volume.
That's true! And why are we prescribing more and more drugs to treat lower and lower thresholds for disease? Because the medical journal editors don't do their jobs:
Here is a classic case of the kind of thing that bedevils the American health system—dubious findings that, without careful evaluation, have the potential to drive up costs. But whose fault is it? It’s hard to blame Pravachol’s manufacturer, Bristol-Myers Squibb. The study’s principal objective was to look at Pravachol’s effectiveness in fighting heart attacks; the company was simply using that patient population to make a secondary observation about strokes. In any case, Bristol-Myers didn’t write up the results. A group of cardiologists from New Zealand and Australia did, and they hardly tried to hide Pravachol’s shortcomings in women and older people. All those data are presented in a large chart on the study’s third page. What’s wrong is the context in which the study’s findings are presented. The abstract at the beginning ought to have been rewritten. The conclusion needs a much clearer explanation of how the findings add to our understanding of stroke prevention. There is no accompanying commentary that points out the extreme cost-ineffectiveness of Pravachol as a stroke medication—and all those are faults of the medical journal’s editorial staff. In the end, the fight to keep drug spending under control is principally a matter of information, of proper communication among everyone who prescribes and pays for and ultimately uses drugs about what works and what doesn’t, and what makes economic sense and what doesn’t—and medical journals play a critical role in this process. As Abramson writes:
"When I finished analyzing the article and understood that the title didn’t tell the whole story, that the findings were not statistically significant, and that Pravachol appeared to cause more strokes in the population at greater risk, it felt like a violation of the trust that doctors (including me) place in the research published in respected medical journals."
The journal in which the Pravachol article appeared, incidentally, was The New England Journal of Medicine. And its editor at the time the paper was accepted for publication? Dr. Marcia Angell. Physician, heal thyself.
Amen, brother. And stop press-releasing those dubious findings to the nation's newspapers!
UPDATE: That last quote in the New Yorker article was from the new book Overdosed America : The Broken Promise of American Medicine, which I happen to be reading at the moment. It's nice to see an academic addressing these issues. And it looks like his ideas are starting to get the attention of the mainstream press.
Enough to Make You Sick: As if there weren't enough disease in the world, researchers, aided and abetted by the U.S. government, are inventing more:
Nearly six in 10 Americans have blood pressure high enough to increase their risk of heart attacks, strokes and kidney problems, according to a study released Monday.
The official cutoff for high blood pressure, which doctors call hypertension, is a reading higher than 140 over 90. Last year, the government added a new risk category, prehypertension, that includes a top number between 120 and 139 or a bottom number between 80 and 89.
The study found that 27 percent of adults have hypertension and 31 percent have prehypertension, for a combined total of 58 percent.
...The Wangs examined data from a government health survey of 4,805 adults conducted in 1999-2000. 'We're facing a very serious challenge,' Youfa Wang said..
The prevalence of hypertension has increased by approximately 10 percentage points during the past decade. The awareness and appropriate management of hypertension among hypertensive patients remain low: 31% were not aware of their disease, only two thirds (66%) were told by health professionals to adopt lifestyle modifications or take drugs to control hypertension, and only 31% controlled their hypertension.
With 60% of the population affected, the United States is facing a serious challenge in the prevention and management of prehypertension and hypertension. People’s awareness and control of hypertension remain poor. This study highlights the seriousness of the problem and the importance of promoting lifestyle modifications.
Let me just say that including this "pre-hypertensive" category makes the problem seem larger than it is. Only 27% of adults actually have hypertension. And doctors aren't ignoring that. It's the silly, hyperventilating category of "pre-hypertension" that we're ignoring. This category came into existence by the grace of the Seventh Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Having run out of useful things to say after Committees 1-6, they came up with this designation, warning that people with normal blood pressure in the range of 120-139/30-39 run the risk of developing high blood pressure with time.
And so they do. Our blood pressure tends to increase as we age. It's really a measure of the elasticity of our arteries. And as we age, we lose that elasticity and the arteries become stiffer. Stiffer arteries mean higher pressure. Stiffer arteries also mean a higher risk of strokes and heart attacks. (You know, "hardening of the arteries.")
The question is, does doing anything about those normal readings in the "pre-hypertension" range make any difference in the long run? We don't know. As long as the "treatment" is benign, such as recommending diet and exercise, it's no big deal. But when researchers start hyperventilating about a widespread problem that isn't really a problem, well, that's a problem.
I'd write more, but the pre-arthritis in my fingers prevents me. Must save them for future use. Instead, go here for another take on the matter. posted by Sydney on
10/27/2004 08:02:00 AM
0 comments
Tuesday, October 26, 2004
Letters: A group of healthcare experts (aka academics) has written a letter to the President, calling him a liar:
Dear Mr. President:
We were among the signers of the statement issued last week by the Health Care Finance Group ( http://www.sunya.net/healthfinance.html). That statement challenged the claim, frequently presented in your speeches and campaign advertising, that your opponent’s health care proposals would amount to a “government take-over” of the health care system and result in “government-run health care.”
The nonpartisan statement, which neither endorses nor rejects any particular approach to health care policy, has been signed by ninety-five of the nation’s leading experts in health policy and health care finance. It makes clear that, whatever the merits of Senator Kerry’s proposals, it is simply not accurate to describe them as you have.
If you believe that we are mistaken, please direct us to any genuine expert in health care policy or health care finance who agrees with your claim, or any genuine analysis that supports it. Otherwise, we would respectfully suggest that it does not serve the nation or honor the office of the presidency to continue to make a charge so obviously contrary to fact.
We all know how non-partisan academia is. And, despite their "over a thousand combined years of experience," they're wrong. Any plan that expands Medicaid to include over 50% of the population - which is what the Kerry plan does - is a plan that involves government take-over of the healthcare system. There's just no getting around it.
UPDATE: People are asking, "where does Kerry say he's going to put over 50% of the population on Medicaid?" His healthcare plan calls for expanding Medicaid coverage to children families that make up to 300% of the federal poverty level. According to the 2004 Federal Poverty Guidelines, 300% of the federal poverty level for a family of four would be a yearly income of $56,500. And according to the U.S. Census Bureau, the median yearly income in 2003 for family households was $53,991. Assuming that the average family is a family of four, that means that over 50% of families would qualify for Medicaid. And believe me, employers won't foot the bill for healthcare insurance when they know their employees can get Medicaid. So a large segment of the population will be shifted to Medicaid, and that's a government healthcare program.
Maybe I'm misinterpreting the statistics. If so, let me know. But, I think far more people would end up being covered by Medicaid than by the re-insurance part of his plan.
UPDATE II: Here's some input:
He wants to expand coverage to kids in families making 300% of poverty.
For adults, it's only 200% of poverty. And it isn't a guaranteed thing,
really. It's a funded agreement that states don't have to buy into if
they don't want.
Forty percent of families make 200% of the poverty level. Add to that the kids in the the 300% families, and you'd probably have a pretty close to 50% Medicaid coverage.
And more:
I have heard many people argue that Medicaid "isn't government run health care". In the strictest sense of the term "government run", they would be correct. The government is not assiging patients particular doctors, directing them when they may see a doctor, etc. Currently, the government cannot impose limits or standards by which the physician and patient must interact. On the other hand, whoever is footing the bill has the final say in care. As spending rises, the one controlling the purse will exact greater control over the distribution of funds. Whether this is in the form of restricted access to care or lower reimbursement for care is up to the government (for some reason I think option #2 would be more likely). To assume that the government would not play a significant role in dispersal of care when it is responsible for the cost of care is just naive.
Alas, these are just the ramblings of a med-student hopeful. Sometimes I wonder if my future colleagues are really this naive, or just misguided by such faculty as the letter-writers. Differing concepts of reality are what make me anxious for the inevitable question of health care policy come Admissions Committee Interviews.
And in a lighter vein:
If you wondered how John Kerry intended to deliver on his pledge of no tax increases while at the same time saving Social Security, providing universal health care, increasing the size of the military, cutting the deficit, and putting a car in every garage, wonder no more!
I have it on good authority that he's managed to get hold of Teresa's Black Amex card! That's the one a step above Platinum. But that doesn't mean that everybody will get a free ride. You have to do your part. So add a bottle of Ketchup a day to the diet of every man, woman and child.
Pre-Election Peek: Walter Olson has a run-down of the prospects for the tort reform ballot initiatives in Wyoming, Oregon, Nevada, and Florida. posted by Sydney on
10/26/2004 09:13:00 PM
0 comments
Grand Rounds V:Grand Rounds is up, a collection healthcare bloggy goodness. Enjoy.
Next week's Grand Rounds (the Election Day edition) will be here, at Medpundit. Please send your contributions to medpundit-at-ameritech.net by Monday, Nov 1, at 9PM. (And you don't have to be a doctor/nurse/student, etc. to participate. Any blogger with a health/medicine -related post is welcome to contribute.)
Notable Notes: Chief Justice William Rehnquist's thyroid cancer surgery is raising a few eyebrows. The press release from the Supreme Court refers to his "tracheotomy." At least one regular reader wonders if the Court confused the term with "thyroidectomy," the usual treatment for thyroid cancer. Elswhere, pundits are speculating that if he had a tracheotomy his cancer must be very bad. It is odd that he would be planning to return to work next Monday after a tracheotomy.
Wouldn't it be horrible if all of the confusion and speculation turned out to be just a mix-up in medical terminology? (Although, I suppose if that were the case, his doctors would have spoken up by now. Unless, of course, they've been too busy...) posted by Sydney on
10/26/2004 08:50:00 AM
0 comments
Stem Cell Q&A: A fair and balanced look at the stem cell debate from the Albany Times Union, reprinted in my morning paper. (Requires registration.) Too bad Newsweek, NPR, The New York Times, and the Washington Post haven't published something like this. posted by Sydney on
10/26/2004 08:31:00 AM
0 comments
Flu Vaccine Update: Craig Westover has an excellent column analyzing the causes behind the flu vaccine shortage, and why that kind of shortage could extend to other medications under a system of federal drug price controls.
Meanwhile, I keep reading that the CDC is working with Aventis-Pasteur and Chiron suppliers to find out who needs the vaccine and to distribute it to those who have high risk patients. I have yet to hear anything from my supplier, Chiron's main distributor in the U.S. What's even more worrisome, the public health department here seems to be as clueless as I am:
Moser expects more vaccine to make its way to Summit County via the drug manufacturer Aventis Pasteur and the U.S. Centers for Disease Control and Prevention, but he can't guarantee that will happen.
Hmm. Maybe I was too premature in my praise for the CDC's plan. They certainly haven't been very good at keeping the lines of communication open with those on the front lines.
Outsourcing Healthcare: England has been recruiting doctors from outside the UK for some time to make up for a physician shortage and cut down on patient waiting times. Matthew Holt notes that some of those recruits are American. He notes that most of them are either doctors who "hit a glass ceiling" or those at the end of their career, but not newly minted doctors. I suppose moving to England and getting paid a salary would be appealing to doctors who are no longer working to support their families. I'm betting most of them are of the near-retirement variety. It would be interesting to know the age break-down and their reasons for signing up.
UPDATE: The Glittering Eye notes a reverse trend - the Sub-Saharan medical braindrain to Western countries, and questions the morality of wealthy nations harvesting the medical minds and bodies of poorer nations. posted by Sydney on
10/26/2004 07:59:00 AM
0 comments
Monday, October 25, 2004
Ugly Ducklings: The naked mole rat may hold the key to understanding pain. I'd never heard of naked mole rats until I saw the movie Fast, Cheap & Out of Control in which one of the documentary's subjects has a life-long fascination with the critters. posted by Sydney on
10/25/2004 08:16:00 PM
0 comments
Takin' It to the People: Four states have ballot initiatives on tort reform in next week's election:
•In Wyoming, a proposed constitutional amendment would allow lawmakers to place a not-yet-determined cap on noneconomic losses.
•In Oregon, noneconomic awards would be capped at $500,000.
•In Florida, where lawmakers imposed a $500,000 cap last year, the proposal would limit attorneys' share of any malpractice settlement to 30 percent at most and less in the case of large awards.
•In Nevada, the measure would remove all exemptions from an existing $350,000 cap and limit attorneys' fees.
Doctors depict the fee limits as an appropriate swipe at greedy lawyers.
"The voters can make their own judgment," Mr. Matheis said. "Is having enough doctors more important than personal-injury lawyers becoming very wealthy?"
Should be interesting to see if they pass and by what margin. If they pass by a large margin that should send a clear signal to the Senate that the will of the people is not the same as the will of the trial lawyer lobby. posted by Sydney on
10/25/2004 07:53:00 AM
0 comments
Pharmacists in England and Wales could offer some health services currently provided by GPs, under a new deal agreed with the government.
These would include supplying repeat prescriptions, offering basic health advice and blood pressure checks.
This was common practice in the 18th and 19th centuries, when the word "doctor" applied to a range of professions of different social standing. The apothecary was the druggist. He was the lowest man on the social totem pole - not only did he touch people, but he was a merchant to boot. Surgeons were a step above - they touched people, but they weren't merchants. More like a skilled tradesman. The most elevated of all was the physician who went to medical school and thus was highly educated but didn't touch people, except to delicately take a pulse. That's why the snobby characters in Jane Austen's novels always referred pointedly to calling "the physician, not the apothecary."
UPDATE: A reader comments:
That's still reflected in British medical customs today. Surgeons are addressed as "Mister"/"Miss"/"Missus". Physicians are addressed as "Doctor".
I note that you don't offer an opinion on the changes they're talking
about. While I'm uncertain about this particular reform, I suspect that serious reform in the practice of medicine is inevitable largely due to technology, educational reforms, and the increasing significance of the healthcare sector in the overall economy. This latter suggests that there will be a significantly increasing number of very educated people in healthcare (as a proportion of the population) who aren't doctors. I'd be surprised if the present practice of medicine can survive this as-is. posted by Sydney on
10/24/2004 09:25:00 PM
0 comments
Documentation Squared: From a review in the British Medical Journal of a book about the trajectory of British Medicine :
The climate of distrust drives demands for reform and further documentation to ensure that doctors are doing their jobs and conforming to the rules. These demands, of course, only increase the obstacles to doctors being able to do their jobs effectively. Tallis notes in an aside, 'Because every document that is generated by the Trust has to be checked against central guidelines, we have to document that our documents meet documenting standards.
Hope: More evidence that this year's flu epidemic will be mild:
Influenza epidemics are notoriously difficult to predict, but experience has shown that the worst seasons are typically those in which an antigenically drifted influenza A virus of the so-called H3 hemagglutinin subtype predominates. Last year’s epidemic, caused mainly by viruses resembling A/Fujian/411/2002 (H3N2), was an example of this phenomenon. To date, no important new H3 virus has been detected through surveillance, so if we are lucky, the impact of the vaccine shortage may be mitigated by a relatively mild influenza season. posted by Sydney on
10/24/2004 08:37:00 PM
0 comments




{kind=link}
{kind=link}
{kind=link}